

The human heart beats approximately 100,000 times every day. The lungs cycle 20,000 breaths. The arterial tree silently propels five litres of blood per minute through 60,000 miles of vessels. When disease threatens any part of this extraordinary system — whether through blocked coronary arteries, diseased heart valves, a rupturing aorta, or a malignant lung mass — it falls to the Cardiothoracic And Vascular Surgery (CTVS) to intervene with precision, knowledge, and the full force of modern surgical science.
As a Cardiothoracic and Vascular Surgeon practising in Bhubaneswar, Odisha, with over fifteen years of experience spanning the complete spectrum of CTVS surgery, I have had the privilege of operating on the heart, the lungs, the great vessels, and the peripheral circulation of thousands of patients across eastern India. In this comprehensive article, I aim to demystify the field of CTVS surgery — its scope, its sub-disciplines, its techniques, and why access to a specialised CTVS surgeon matters profoundly to patients across Odisha and beyond.
What Is Cardiothoracic & Vascular Surgery?
Cardiothoracic and Vascular Surgery, universally abbreviated as CTVS, is a surgical super-specialty that encompasses the operative management of diseases affecting three intimately related anatomical domains:
• The Cardiac Domain — the heart and its valves, coronary arteries, pericardium, and intracardiac structures
• The Thoracic Domain — the lungs, pleura, oesophagus, trachea, mediastinum, and chest wall
• The Vascular Domain — the aorta, its major branches, peripheral arteries and veins, and the lymphatic system
A CTVS surgeon or a CTVS Specialist must command not only the technical dexterity to operate within the thoracic cavity and on beating or arrested hearts, but also a deep mastery of cardiovascular physiology, haemodynamic monitoring, cardiopulmonary bypass technology, intensive care management, and the rapidly evolving landscape of hybrid and endovascular interventions. It is, in every sense, the most demanding and consequential of surgical super-specialties.
The Cardiac Surgery Domain — Operating on the Heart
Coronary Artery Bypass Grafting (CABG)
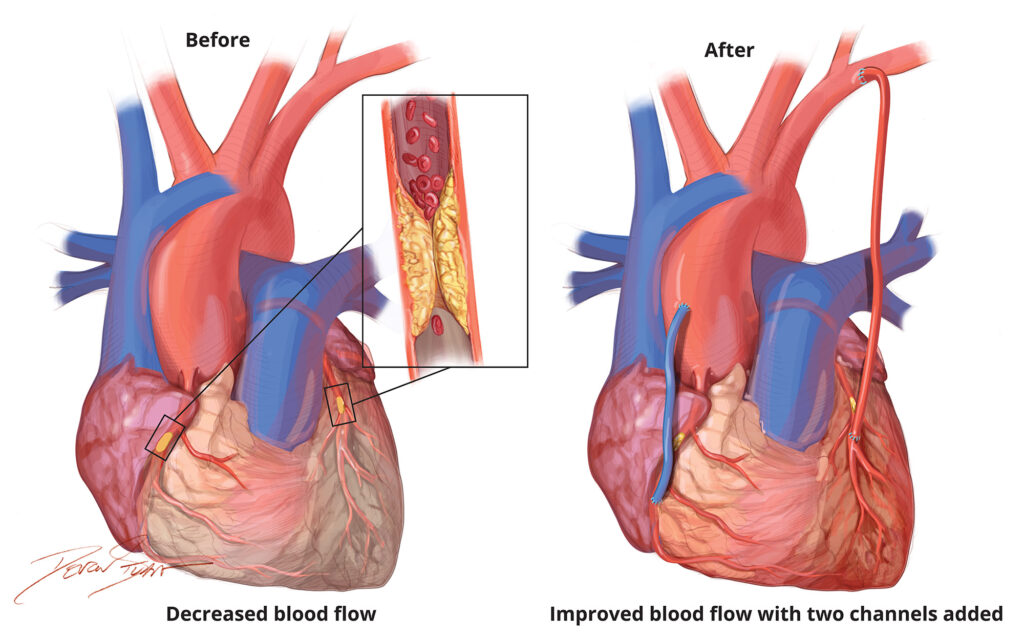
Coronary Artery Disease (CAD) remains the leading cause of death in India and globally. When coronary arteries are occluded by atherosclerotic plaque — narrowing the vessel lumen and starving the myocardium of oxygenated blood — Coronary Artery Bypass Grafting (CABG) is the definitive surgical solution.
In CABG, healthy conduit vessels are harvested from elsewhere in the patient's body and anastomosed distal to the coronary obstruction, creating a biological bypass channel that restores myocardial perfusion. The three principal conduits are:
• Left Internal Thoracic Artery (LITA) — anastomosed to the Left Anterior Descending (LAD) artery, the gold standard with patency rates of 95–98% at ten years
• Saphenous Vein Graft (SVG) — harvested from the leg using endoscopic or open technique; workhorse conduit for multi-vessel disease
• Radial Artery Graft — harvested from the non-dominant forearm; superior long-term patency compared to saphenous vein
CABG may be performed on-pump (with cardiopulmonary bypass and cardiac arrest under cold crystalloid or blood cardioplegia) or off-pump (OPCAB — on the beating heart using mechanical stabiliser devices), depending on patient anatomy, ventricular function, and co-morbidity profile. Total arterial revascularisation — bypassing all diseased vessels with arterial conduits — represents the highest standard of contemporary CABG, offering superior long-term event-free survival.
Heart Valve Surgery — Repair and Replacement
The four cardiac valves — mitral, aortic, tricuspid, and pulmonary — govern the unidirectional flow of blood through the cardiac chambers. Valve disease manifests as either stenosis (failure to open adequately, obstructing forward flow) or regurgitation (failure to close completely, causing retrograde leak) — or frequently, a combination of both.
**Mitral Valve Surgery** is the most frequently performed valve operation in India, where rheumatic heart disease remains endemic. Mitral valve repair — when anatomically feasible — is strongly preferred over replacement, employing techniques of leaflet resection, neochord implantation using expanded polytetrafluoroethylene (ePTFE) sutures, commissurotomy, and prosthetic ring annuloplasty. Repair is associated with superior long-term survival, preserved left ventricular function, and the avoidance of lifelong anticoagulation.
**Aortic Valve Surgery** involves either replacement of the diseased aortic valve with a mechanical prosthesis (St. Jude Medical bileaflet or On-X valve) or a biological tissue valve (porcine or bovine pericardial bioprosthesis). The Ross Procedure — transplanting the patient's own pulmonary valve to the aortic position and replacing the pulmonary valve with a homograft — offers the ideal solution for younger patients requiring aortic valve replacement, providing a living autograft with haemodynamic performance superior to any prosthesis.
**Tricuspid Valve Surgery** typically involves annuloplasty (ring repair) for functional tricuspid regurgitation secondary to right ventricular dilatation, commonly performed concomitantly with mitral or aortic procedures.
Surgery for the Aorta — The Body's Great Artery
The aorta — the largest artery in the human body — is the primary conduit of oxygenated blood from the left ventricle to the systemic circulation. Diseases of the aorta represent some of the most dramatic and life-threatening presentations in cardiovascular medicine.
Aortic Aneurysm is a pathological dilatation of the aortic wall beyond 1.5 times its normal diameter, caused by medial degeneration, atherosclerosis, connective tissue disorders (Marfan syndrome, Ehlers-Danlos syndrome), or inflammatory aortitis. Surgical repair — either open (Dacron interposition graft replacement) or endovascular (TEVAR/EVAR using stent grafts delivered percutaneously) — is indicated when the aneurysm reaches the critical threshold of 5.5 cm for the descending thoracic aorta or 5.0 cm for the ascending aorta, or when the growth rate exceeds 0.5 cm per year.
Acute Aortic Dissection — a catastrophic tear in the aortic intima through which blood forcibly penetrates, creating a false lumen — demands emergency surgical intervention for Type A dissection (involving the ascending aorta) and carefully selected endovascular intervention for Type B dissection. Ascending aortic replacement under hypothermic circulatory arrest with antegrade cerebral perfusion remains the cornerstone of Type A dissection surgery and demands the highest level of surgical and perfusionist expertise.
Congenital heart defects — structural abnormalities present at birth — affect approximately 8 per 1,000 live births in India. CTVS surgeons operating in the congenital domain perform a diverse array of palliative and corrective procedures including:
• Closure of Atrial Septal Defects (ASD) and Ventricular Septal Defects (VSD)
• Repair of Tetralogy of Fallot (TOF) — the most common cyanotic congenital heart defect
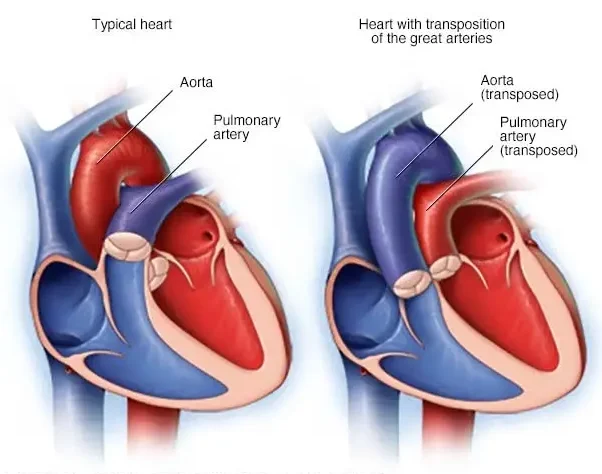
• Arterial Switch Operation for Transposition of the Great Arteries
• Glenn and Fontan procedures for univentricular heart physiology
• Surgical repair of coarctation of the aorta and patent ductus arteriosus (PDA)
The integration of paediatric cardiac surgery with interventional cardiology in hybrid catheterisation laboratories has expanded treatment options for complex congenital lesions previously considered inoperable.
The Thoracic Surgery Domain — Chest and Lung Operations
Lung Surgery — Resection and Reconstruction
Pulmonary surgical disease encompasses malignant (primary and metastatic lung cancer), infective (bronchiectasis, pulmonary aspergillosis, destroyed lung), and structural (emphysematous bullae, spontaneous pneumothorax) pathology. Operative procedures include:
• **Lobectomy** — resection of an entire pulmonary lobe; the standard oncological resection for non-small cell lung cancer (NSCLC) Stage I–IIIA
• **Pneumonectomy** — removal of an entire lung; reserved for centrally located tumours involving the main bronchus or pulmonary vessels
• **Segmentectomy and Wedge Resection** — anatomical or non-anatomical lung-sparing resections for small peripheral lesions in patients with compromised pulmonary reserve
• **Decortication** — surgical stripping of the fibrous peel enveloping a trapped lung in chronic empyema thoracis
• **Bullectomy** — resection of giant emphysematous bullae compressing adjacent functional lung tissue
Video-Assisted Thoracoscopic Surgery (VATS) has transformed thoracic surgical oncology. VATS lobectomy — performed through three or four ports of 5–12 mm without rib spreading — achieves equivalent oncological resection to open thoracotomy with significantly reduced post-operative pain, blood loss, and pulmonary complication rates.
Oesophageal Surgery
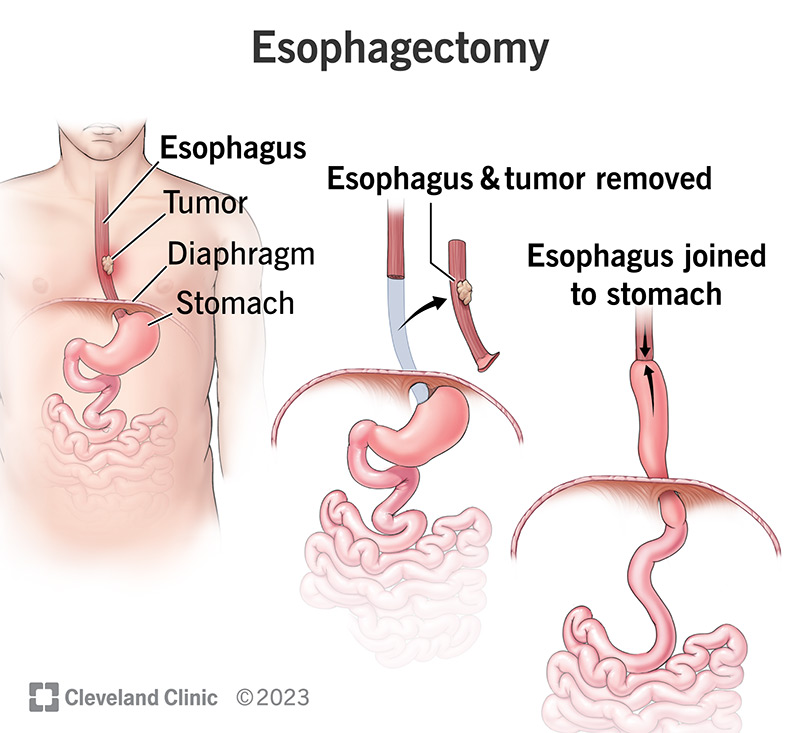
Cancer of the oesophagus carries a dismal prognosis when diagnosed late and demands surgical resection as the only potentially curative intervention. Oesophagectomy — the surgical removal of the diseased oesophagus with reconstruction using a gastric conduit, colonic interposition, or jejunal graft — is one of the most technically demanding operations in thoracic surgery. The minimally invasive Ivor Lewis oesophagectomy, combining laparoscopic abdominal mobilisation with thoracoscopic thoracic dissection and high intrathoracic anastomosis, has become the operative standard in experienced centres.
Mediastinal and Pleural Surgery
The mediastinum — the central compartment of the thorax housing the heart, great vessels, trachea, oesophagus, and thymus — is the site of diverse tumours including thymoma, germ cell tumours, lymphoma, and neurogenic masses. Surgical resection via sternotomy, thoracotomy, or VATS is undertaken based on tumour location, size, and histological subtype. Pleural mesothelioma — malignancy of the pleural lining — may be managed with extended pleurectomy and decortication (P/D) in selected cases.
The Vascular Surgery Domain — Arteries, Veins, and Beyond
Peripheral Arterial Disease and Bypass Surgery
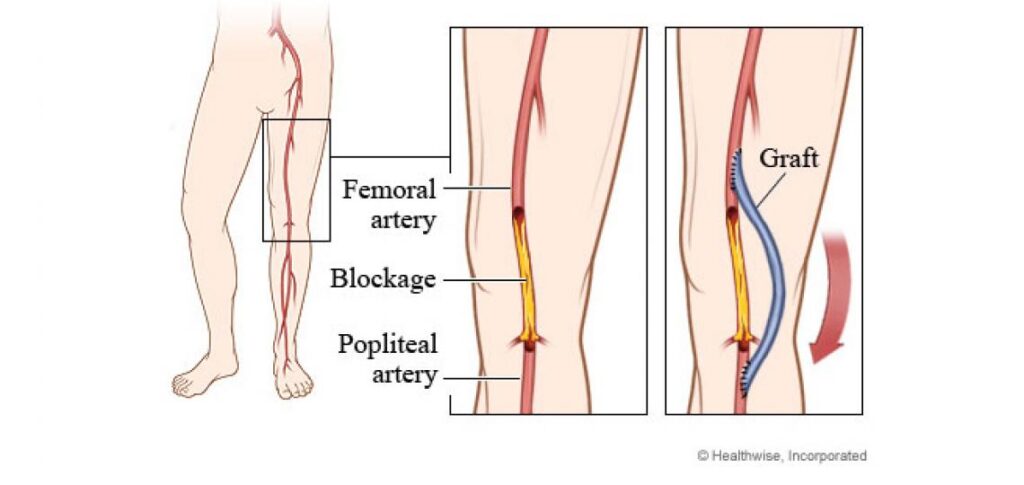
Peripheral Arterial Disease (PAD) — caused by atherosclerotic obstruction of limb arteries — produces a clinical spectrum from intermittent claudication to critical limb-threatening ischaemia (CLTI) with rest pain, non-healing ulcers, and imminent gangrene. Surgical management includes:
• **Femoropopliteal Bypass** — using reversed saphenous vein or prosthetic (PTFE) graft to revascularise the ischaemic limb below an occlusive iliac or femoral lesion
• **Aorto-Bifemoral Bypass** — for aorto-iliac occlusive disease (Leriche syndrome), restoring inflow to both lower extremities
• **Profundaplasty** — reconstruction of the profunda femoris artery origin to augment collateral circulation
Hybrid vascular procedures — combining open surgical reconstruction with intraoperative balloon angioplasty and stenting — have extended revascularisation options for patients with complex multi-level disease.
Carotid Artery Surgery — Stroke Prevention
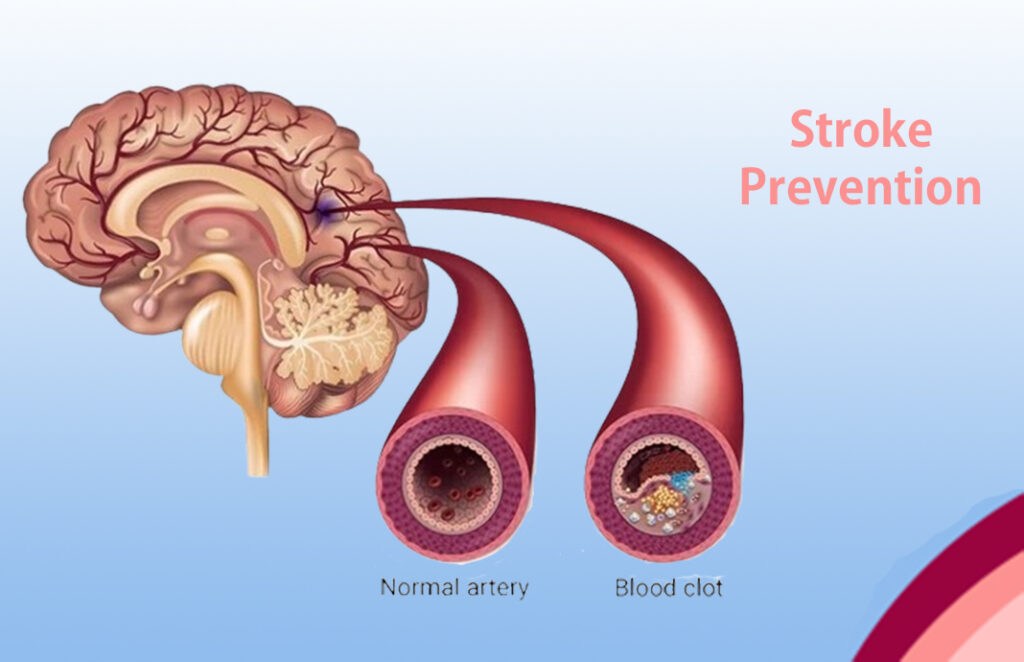
Carotid artery stenosis — most commonly due to atherosclerotic plaque at the carotid bifurcation — is the leading surgically treatable cause of ischaemic stroke. Carotid Endarterectomy (CEA) — surgical removal of the atheromatous plaque under regional or general anaesthesia with intraoperative neuromonitoring — reduces the five-year ipsilateral stroke risk by over 50% in symptomatic patients with stenosis exceeding 70% of the vessel diameter.
Venous Disease — Varicose Veins and Deep Vein Thrombosis
Chronic venous insufficiency manifests as varicose veins, venous ulceration, and post-thrombotic syndrome. Surgical management encompasses saphenofemoral junction ligation and great saphenous vein stripping, laser endovenous ablation (EVLA), radiofrequency ablation (RFA), and ultrasound-guided foam sclerotherapy. Surgical thrombectomy and catheter-directed thrombolysis are employed for acute iliofemoral deep vein thrombosis to prevent post-thrombotic syndrome and pulmonary embolism.
Why Choose a Dedicated CTVS Surgeon in Bhubaneswar?
Odisha carries a significant burden of rheumatic heart disease, coronary artery disease, peripheral vascular disease, and thoracic malignancy. Until recently, patients requiring advanced CTVS procedures were compelled to travel to Chennai, Kolkata, or Delhi — uprooting families, incurring enormous financial burden, and losing precious time in time-critical surgical emergencies.
The establishment of dedicated CTVS surgical programmes in Bhubaneswar has fundamentally transformed cardiac and vascular surgical access for the people of Odisha and neighbouring states including Chhattisgarh, Jharkhand, and Andhra Pradesh. With over fifteen years of practice in Bhubaneswar, I have operated on patients across this region — restoring hearts, saving limbs, removing lung cancers, and repairing aortas — with outcomes that compare favourably with the finest tertiary cardiac centres in the country.
Advanced perioperative infrastructure — including dedicated cardiac intensive care units, real-time intraoperative transoesophageal echocardiography, on-site perfusion teams, hybrid operating theatres, and multidisciplinary heart team conferences — ensures that patients in Bhubaneswar receive world-class CTVS surgical care without leaving their home state.
Schedule Your Appointment : For Expert Care
Contact Dr. Jhulana Jena Today
Phone: +91 99304 06067
Call to schedule an appointment or discuss your concerns. The clinic staff will help you find a convenient consultation time.
Email: jhulanajena@yahoo.com
Send your inquiries or request an appointment via email. You can also share relevant medical records for review before your visit.
Clinic Location:
Room 33,
Cardiology OPD Block ,
Ground Floor,Utkal Hospital
Get Directions: https://maps.app.goo.gl/MC81q1cFi5JgtMV97
Easily accessible location with convenient parking. The clinic is well-connected by public transport and private vehicles.
Frequently Asked Questions (FAQ) — CTVS Surgery
What is CTVS surgery?
CTVS (Cardiothoracic and Vascular Surgery) is a surgical super-specialty covering operative treatment of heart disease, lung disease, oesophageal disease, aortic pathology, and peripheral vascular disease. Procedures range from coronary bypass and valve surgery to lung resection and aortic aneurysm repair.
How do I know if I need CTVS surgery?
You should consult a CTVS Specialist if you have been diagnosed with significant coronary artery disease not amenable to stenting, severe valve disease (stenosis or regurgitation), aortic aneurysm or dissection, lung cancer, oesophageal cancer, or peripheral arterial disease causing limb-threatening ischaemia. Your cardiologist or physician will provide a referral based on your diagnostic reports.
Is heart surgery safe in Bhubaneswar?
Yes. Bhubaneswar has world-class cardiac surgical facilities with experienced CTVS surgeons and CTVS Specialist, dedicated cardiac ICUs, and advanced intraoperative monitoring.Dr. Jhulana Kumar Jena's practice offers surgical outcomes consistent with national and international standards.
What is the difference between a cardiologist and a CTVS surgeon?
A cardiologist is a physician who diagnoses and manages heart disease medically and performs interventional procedures such as angioplasty and stenting. A CTVS surgeon is a surgical specialist who operates on the heart, lungs, and blood vessels when medical or interventional management is insufficient. Both work together within a multidisciplinary heart team.
How long does recovery take after heart surgery?
Recovery after conventional cardiac surgery (CABG or valve surgery) involves 7–10 days of hospitalisation and 6–12 weeks to full recovery. Minimally invasive procedures reduce hospital stay to 3–5 days and full recovery to 2–4 weeks.
What is the cost of CTVS surgery in Bhubaneswar?
The cost of CTVS procedures in Bhubaneswar varies based on the type of surgery, prosthesis used, and duration of ICU stay. Many procedures are covered under Ayushman Bharat PM-JAY and Biju Swasthya Kalyan Yojana (BSKY), making advanced cardiac surgical care accessible to economically vulnerable patients across Odisha. Contact the hospital for procedure-specific cost estimates.
Conclusion — The CTVS Surgeon's Commitment to Odisha
Cardiothoracic and Vascular Surgery stands at the intersection of human biology's most vital systems and the highest expression of surgical craft. Every CABG restores myocardial perfusion to a heart on the edge of failure. Every valve repair returns a damaged mitral or aortic valve to lifelong physiological function. Every aortic repair prevents a catastrophic rupture. Every lobectomy offers a lung cancer patient the chance of cure. Every peripheral bypass saves a limb and a livelihood.
For fifteen years, it has been my deepest professional commitment to bring this level of CTVS surgical expertise to the patients of Bhubaneswar and all of Odisha — ensuring that geography is no longer a barrier to life-saving cardiac, thoracic, and vascular surgical care. Whether you are a patient newly diagnosed with coronary artery disease, a family member seeking the best surgical opinion for a loved one with a leaking heart valve, or a referring physician exploring surgical options for a complex vascular case — I invite you to engage with our team and experience the standard of CTVS care that every patient deserves.