

Cardiac surgery has undergone a paradigm shift. What once required a twelve-inch sternotomy, weeks in the intensive care unit, and months of rehabilitation can today be accomplished through keyhole incisions the width of a fingertip — with patients returning home in days. This is the promise, and now the proven reality, of Minimally Invasive Cardiac Surgery.
As a practising Cardio Thoracic and Vascular Surgeon with over fifteen years of dedicated experience in Minimally Invasive Cardiac Surgery (MICS) at tertiary cardiac centres in Odisha, I have witnessed firsthand how this discipline has redefined what is surgically possible — and what patients can expect from their recovery.
Foundation
What Is Minimally Invasive Cardiac Surgery?

Minimally Invasive Cardiac Surgery is an umbrella term encompassing a diverse range of cardiac operative techniques performed through incisions substantially smaller than those required for conventional median sternotomy — typically ranging from 2 to 6 centimetres. Rather than splitting the sternum longitudinally to gain wide access to the mediastinum, MICS utilises alternative thoracic entry points — including mini-thoracotomy, parasternal incisions, and sub-xiphoid approaches — often augmented by specialised instrumentation, video-assisted thoracoscopy (VATS), robotic platforms, and advanced percutaneous cannulation strategies for cardiopulmonary bypass.
The philosophical core of MICS is the principle of tissue economy: achieving complete, durable surgical correction of cardiac pathology while minimising the collateral trauma inflicted on the chest wall, sternal architecture, intercostal musculature, and the attendant inflammatory cascade. This translates directly into reduced intraoperative blood loss, diminished post-operative pain, accelerated pulmonary function recovery, and measurably superior patient-reported quality-of-life outcomes.
Spotlight Procedure

Minimally Invasive Mitral Valve Surgery: The Gold Standard Benchmark
Among all MICS procedures, minimally invasive mitral valve repair via right anterolateral mini-thoracotomy has emerged as the most widely performed and comprehensively studied. Utilising a 4–6 cm incision in the right fourth intercostal space, combined with femoro-femoral cardiopulmonary bypass, endoballoon aortic occlusion or transthoracic aortic clamping, and carbon dioxide field flooding to prevent air embolism, the surgeon gains excellent visualisation of the mitral apparatus through video-endoscopic magnification.
The operative strategy mirrors open mitral surgery in its completeness: quadrangular or triangular resection of the prolapsing posterior leaflet, Gore-Tex neochord implantation for anterior leaflet pathology, ring annuloplasty with a semi-rigid prosthetic ring, and intraoperative transoesophageal echocardiography (TOE)-guided assessment of repair adequacy. Repair rates exceeding 95% for degenerative mitral regurgitation are consistently achievable in high-volume MICS centres.
Technical Considerations: Peripheral Cannulation & Myocardial Protection

Peripheral cannulation via the femoral vessels remains the cornerstone of minimally invasive cardiopulmonary bypass. The femoral artery is cannulated with a wire-guided Bio-Medicus arterial cannula (15–17 Fr), while femoral venous cannulation employs a long, multi-stage venous cannula advanced under transoesophageal echo guidance into the right atrium and superior vena cava.
Myocardial protection is achieved through antegrade cold blood cardioplegia delivered via a transthoracic aortic root cannula, supplemented by retrograde cardioplegia through a coronary sinus catheter when dictated by coronary anatomy. Cold topical irrigation and systemic hypothermia to 28–32°C provide additional myocardial quiescence during the ischaemic interval.
“In my fifteen years of operating on the heart through incisions smaller than a patient’s palm, what never diminishes is the privilege — and the responsibility — of restoring a life through the smallest possible wound.”
— Dr. Jhulana Kumar Jena, Cardio Thoracic Surgeon, Bhubaneswar.
Clinical Decision-Making
Patient Selection and Preoperative Assessment
Meticulous patient selection is the bedrock of safe and successful MICS. Not every patient with cardiac pathology is an ideal candidate for a minimally invasive approach, and the decision requires a multidisciplinary heart team evaluation incorporating the cardiac surgeon, interventional cardiologist, cardiac anaesthesiologist, and intensivist.
Ideal Candidates for MICS
Isolated mitral or aortic valve disease without concomitant significant coronary artery disease.
Atrial septal defects (ostium secundum) and other structural septal anomalies.
Redo cardiac surgery (avoiding previously scarred mediastinum).
Obesity — where conventional sternotomy carries high wound complication risk.
Patients in vocations requiring early return to activity (musicians, athletes, professionals)
Younger patients with decades of active life ahead desiring cosmetically favourable outcomes.
Relative Contraindications
Severe peripheral arterial disease precluding safe femoral cannulation, significant aortic atherosclerosis with the risk of retrograde embolisation, prior right-sided thoracic surgery with dense adhesions, and severe pulmonary dysfunction necessitating single-lung ventilation precautions are among the relative contraindications that must be carefully weighed by the surgical team.
Preoperative CT angiography of the aorto-iliac vasculature has become mandatory in our practice to map femoral vessel calibre, the presence of atherosclerotic plaque, and any anatomical aberrancy that may complicate peripheral cannulation. Transoesophageal echocardiography and cardiac MRI complete the structural assessment to delineate pathology and guide operative planning.
Coronary Artery Disease
MIDCAB and the Hybrid Revascularisation Paradigm
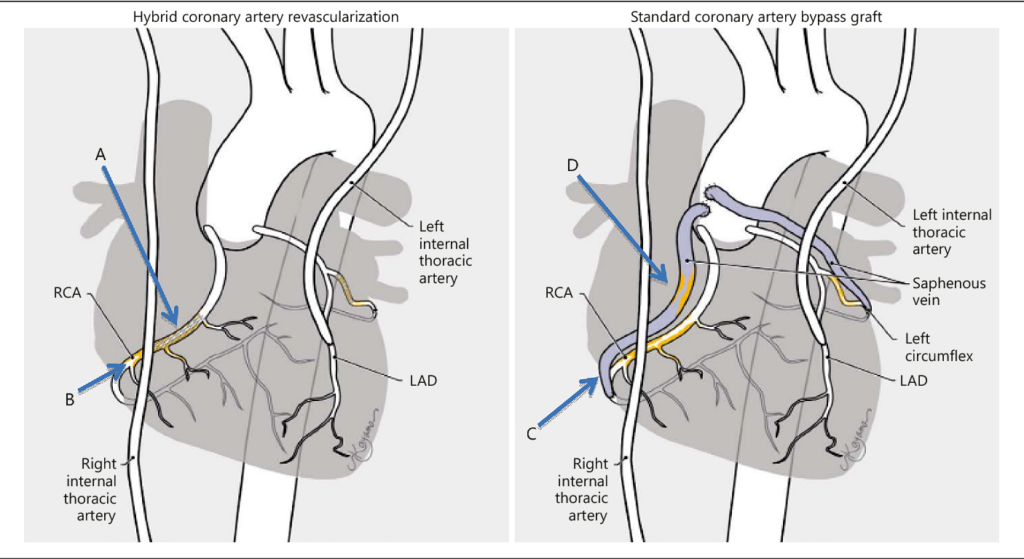
Minimally Invasive Direct Coronary Artery Bypass (MIDCAB) represents the application of MICS philosophy to coronary revascularisation. Performed through a 4–5 cm left antero-lateral mini-thoracotomy between the fourth and fifth ribs, the procedure enables direct visualisation and harvesting of the Left Internal Thoracic Artery (LITA) under direct vision or video-thoracoscopic assistance, followed by off-pump anastomosis to the Left Anterior Descending (LAD) coronary artery using a stabiliser device.
LITA-LAD conduit patency rates in MIDCAB equal those of conventional CABG in the range of 95–98% at ten years with the critical advantage of avoiding cardiopulmonary bypass and its attendant systemic inflammatory response, coagulopathy, and neurocognitive sequelae. For patients with isolated LAD disease and borderline left ventricular function, MIDCAB represents a particularly compelling surgical option.
The Hybrid Coronary Revascularisation (HCR) strategy extends the MIDCAB concept further. The LITA-LAD anastomosis — the most durable revascularisation strategy known to medicine — is performed surgically through a mini-thoracotomy. Non-LAD coronary territories are treated contemporaneously or in a staged fashion with percutaneous coronary intervention (PCI) and drug-eluting stents. This synergistic approach offers complete revascularisation while limiting operative trauma to a minimum.
The Cutting Edge
Robotic-Assisted Cardiac Surgery: Precision at the Nanoscale
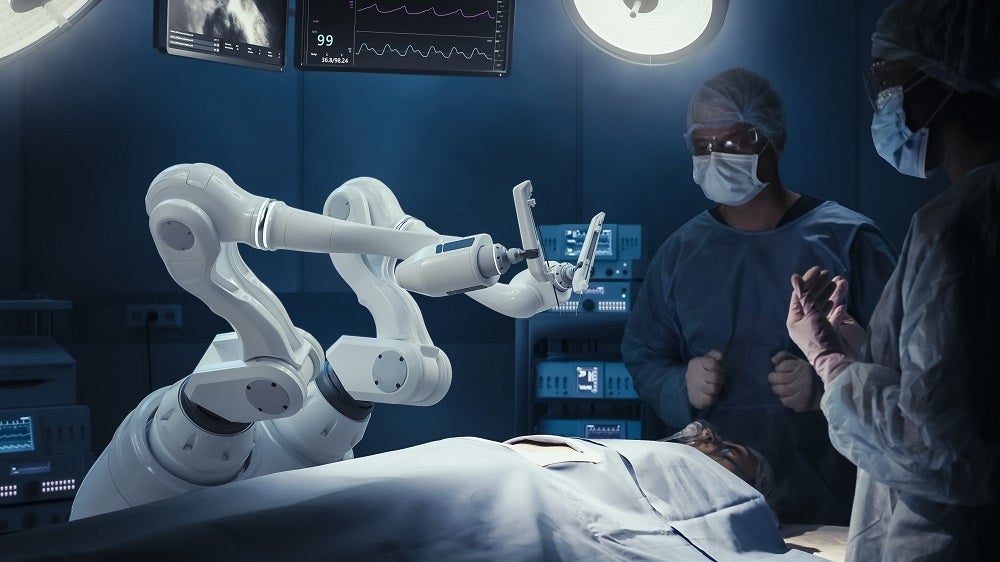
The integration of robotic surgical platforms — principally the da Vinci Surgical System — into cardiac surgery represents the apotheosis of minimally invasive technique. Robotic cardiac surgery (RCS) enables the operating surgeon to perform complex intracardiac procedures through three to four ports of 8–12 mm diameter, seated at a console that provides seven-degrees-of-freedom instrument articulation, 10–15× three-dimensional magnification, and tremor filtration that exceeds the dexterity of the unaided human hand.
Robotic platforms currently find their most compelling cardiac application in mitral valve repair, where the magnified endoscopic view of the subvalvular apparatus allows precise neochord placement, leaflet resection, and ring annuloplasty with exactitude unmatched in any other surgical modality. Robotic ASD closure, totally endoscopic CABG (TECAB), and robotic epicardial ablation for atrial fibrillation represent the expanding frontiers of this technology.
Advantages of the Robotic Platform in MICS
Ergonomic precision: Wristed instrumentation replicates and amplifies natural wrist movement, enabling suturing and knot-tying in anatomically confined spaces with unparalleled control.
Optical superiority: Three-dimensional, high-definition endoscopic visualisation at 10–15× magnification reveals anatomical detail invisible to the naked eye under open-field conditions.
Reproducibility: Digital motion scaling (3:1 or 5:1) eliminates physiological tremor, making each operative movement a deliberate, scaled translation of surgeon intent.
Rhythm Restoration
Thoracoscopic Surgery for Atrial Fibrillation
Atrial fibrillation (AF), the most prevalent sustained cardiac arrhythmia with a prevalence exceeding 1% of the global population, is increasingly amenable to surgical cure through minimally invasive thoracoscopic approaches. In patients with paroxysmal or persistent AF who have failed catheter ablation, thoracoscopic surgical ablation using bipolar radiofrequency energy, microwave, or cryothermy achieves durable pulmonary vein isolation (PVI) and creation of lesion sets replicating the surgical Cox-Maze III procedure.
The bilateral thoracoscopic approach uses three ports per side (5–12 mm), with the patient positioned supine or in a modified lateral decubitus position. Epicardial ablation clamps encircle the pulmonary vein antrum under thoracoscopic vision, delivering high-intensity bipolar energy to create full-thickness, transmural lesion lines that interrupt the re-entrant circuits sustaining AF. Additional lesion sets — including the roof line, inferior line, and left atrial appendage isolation — complete the surgical Maze architecture.
Freedom from AF at five years following thoracoscopic surgical ablation ranges from 70–85% for paroxysmal AF and 60–75% for persistent AF, substantially superior to catheter ablation alone — with the minimally invasive approach ensuring rapid recovery and minimal peri-operative morbidity.
Evidence & Outcomes
Clinical Outcomes and the Evidence Base
The evidence supporting MICS across its procedural spectrum is now robust and drawn from large-volume institutional series, propensity-matched cohort studies, and prospective registries. When performed in experienced centres by dedicated MICS surgeons, outcomes are unambiguously equivalent — and in several specific parameters, superior — to conventional open cardiac surgery.
Key Outcome Domains Where MICS Excels
Blood conservation: Reduced mediastinal dissection and avoidance of sternal marrow exposure translates to 60–70% reduction in allogeneic blood transfusion requirements, lowering transfusion-related immunomodulation, infection risk, and hospital costs.
Pulmonary Function: Preservation of sternal integrity maintains chest wall mechanics, enabling significantly faster recovery of forced expiratory volume and functional respiratory capacity in the post-operative period.
Neurological outcomes: In off-pump MICS procedures, absence of aortic manipulation reduces the incidence of stroke and subclinical neurocognitive decline compared to conventional on-pump surgery with aortic cross-clamping.
Wound morbidity: Deep sternal wound infection — a devastating complication occurring in 3–5% of conventional sternotomies — is virtually eliminated.
Patient satisfaction and cosmesis: Consistently higher patient-reported satisfaction scores, with particular significance for younger and professionally active patients
Tomorrow’s Medicine
The Future of MICS: AI, Imaging, and the Next Frontier
The evolution of MICS is far from complete. Several transformative technologies are poised to redefine the boundaries of minimally invasive cardiac surgery.
Artificial intelligence and machine learning are being integrated into intraoperative imaging platforms to provide real-time echocardiographic interpretation, haemodynamic modelling, and predictive analytics that assist the surgeon in decision-making at critical operative junctures. AI-enhanced annuloplasty ring sizing, automated neochord length calculation, and intraoperative repair durability assessment are amongst the applications under active development.
Augmented reality (AR) surgical navigation — overlaying pre-operative CT and MRI anatomical reconstructions onto the live thoracoscopic field — promises to provide surgeons with a three-dimensional anatomical map that transcends the limitations of two-dimensional endoscopic imaging. Combined with haptic-feedback robotic instruments, this technology will enable surgical precision beyond what is currently achievable.
Transcatheter and hybrid structural heart interventions — including Transcatheter Aortic Valve Implantation (TAVI), MitraClip™ edge-to-edge mitral repair, and transcatheter tricuspid interventions — represent the most catheter-based extension. These technologies expand the treatment envelope to patients considered prohibitive surgical risk, working in concert with surgical MICS to form a comprehensive, risk-stratified structural heart programme.
Closing Perspective
A Surgeon’s Perspective: Why MICS Matters in Odisha
Bhubaneswar and the wider Odisha region have seen a dramatic increase in the burden of rheumatic and degenerative heart disease over the past two decades. For the patients of this region — many of whom are agriculturally employed, economically active, and the primary breadwinners of their families — a shorter hospital stay, faster return to work, and reduced complication burden is not merely a clinical preference. It is an economic and social imperative.
Over fifteen years of MICS practice at tertiary centres serving eastern India, I have had the privilege of restoring cardiac function through incisions smaller than the length of a wristwatch, discharging patients to their families in days. That is the gift of minimally invasive cardiac surgery — and it is one that every eligible patient deserves access to.
As MICS technology emerges it brings the highest standard of minimally invasive cardiac surgical care to the people of eastern India.
Consult Dr. Jhulana Kumar Jena
For a specialised evaluation of your cardiac, schedule a consultation today.
Phone: +91 99304 06067
Call to schedule an appointment or discuss your concerns. The clinic staff will help you find a convenient consultation time.
Email: jhulanajena@yahoo.com
Send your inquiries or request an appointment via email. You can also share relevant medical records for review before your visit.
Clinic Location:
Room 33,
Cardiology OPD Block ,
Ground Floor,Utkal Hospital
Get Directions: https://maps.app.goo.gl/MC81q1cFi5JgtMV97
Easily accessible location with convenient parking. The clinic is well-connected by public transport and private vehicles.
Dr. Jhulana Kumar Jena · MS, MCh (CTVS) · Cardio Thoracic & Vascular Surgeon.
Bhubaneswar, Odisha, India · 15+ Years MICS Experience.